Download as pptx, pdf, or txt
You might also like
- VanGogh EbookDocument288 pagesVanGogh EbookDragan Cvetkovic88% (8)
- Section 13 of HMADocument11 pagesSection 13 of HMAria rajeevNo ratings yet
- Grey AlienDocument7 pagesGrey AlienMKostyakov100% (1)
- Antiepileptics PD 501Document27 pagesAntiepileptics PD 501SidraNo ratings yet
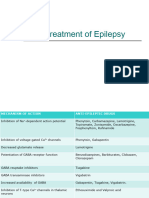
- Drug Treatment of EpilepsyDocument81 pagesDrug Treatment of EpilepsyAnifowose SamsonNo ratings yet
- Medication Summary TLEDocument3 pagesMedication Summary TLEAnastasia Widha SylvianiNo ratings yet
- Bipolar Disorders and Carbamazepine PharmacokinetiDocument6 pagesBipolar Disorders and Carbamazepine PharmacokinetiluthfiahNo ratings yet
- Bipolar Disorders and Carbamazepine PharmacokinetiDocument5 pagesBipolar Disorders and Carbamazepine PharmacokinetiAgr YuroNo ratings yet
- Eti Nurwening Sholikhah: Department of Pharmacology & Therapy Faculty of Medicine Universitas Gadjah MadaDocument43 pagesEti Nurwening Sholikhah: Department of Pharmacology & Therapy Faculty of Medicine Universitas Gadjah MadaadystiNo ratings yet
- Anti EpilepticsDocument29 pagesAnti Epilepticskeerthi sivayanamaNo ratings yet
- Pharmacology of CNS: Prajogo Wibowo Faculty of Medicine Hang Tuah UniversityDocument37 pagesPharmacology of CNS: Prajogo Wibowo Faculty of Medicine Hang Tuah UniversityIda Bagus Putu SwabawaNo ratings yet
- Anti Epileptic DrugsDocument89 pagesAnti Epileptic DrugsInderjeet SohalNo ratings yet
- Anti Seizure Drugs 07Document27 pagesAnti Seizure Drugs 07ashokvishnoi29pNo ratings yet
- Seizure MedicationsDocument3 pagesSeizure Medicationsm.dhiyarahadianNo ratings yet
- Mayra Pagan: Pharmacology-NursingDocument50 pagesMayra Pagan: Pharmacology-NursingmayraNo ratings yet
- 24 Antiseizure DrugsDocument71 pages24 Antiseizure DrugsThea MallariNo ratings yet
- SPC Pramipexole 0.7 MGDocument14 pagesSPC Pramipexole 0.7 MGJehan SarahdiniNo ratings yet
- Antiseizure Drugs - RevDocument17 pagesAntiseizure Drugs - RevGalang Kharisma PutraNo ratings yet
- Epilepsy Part 2Document24 pagesEpilepsy Part 2Sara AbbasNo ratings yet
- Bimbel Ukmppd FarmakoDocument92 pagesBimbel Ukmppd FarmakoJavier AntaresNo ratings yet
- Drugs That Act On The CNSDocument27 pagesDrugs That Act On The CNSnur rachmad afandiNo ratings yet
- Anticonvulsant Part2Document35 pagesAnticonvulsant Part2Rameez ShamounNo ratings yet
- AntiepilepticsDocument13 pagesAntiepilepticstbuyinza21apNo ratings yet
- Adjuvant Analgesics For Pain Management FINAL PARTDocument13 pagesAdjuvant Analgesics For Pain Management FINAL PARTbalamuruganNo ratings yet
- Parkinson Drug TherapyDocument20 pagesParkinson Drug Therapympl.raol50% (2)
- NO. 16. Ayano G (2016) Bipolar Disorders and Valproate PharmacokineticsDocument5 pagesNO. 16. Ayano G (2016) Bipolar Disorders and Valproate PharmacokineticsVincent AriesNo ratings yet
- Antiseizure DrugsDocument55 pagesAntiseizure Drugsswapnali chouguleNo ratings yet
- 3, Antiepileptic DrugsDocument39 pages3, Antiepileptic DrugsAbebe TilahunNo ratings yet
- INTRODUCTION - The Array of Pharmacologic and Surgical Treatments Available For TheDocument4 pagesINTRODUCTION - The Array of Pharmacologic and Surgical Treatments Available For TheKidu GideyNo ratings yet
- NitrazepamDocument4 pagesNitrazepamJunilaNo ratings yet
- 29880020: Antiepileptic Drugs in Critically Ill PatientsDocument12 pages29880020: Antiepileptic Drugs in Critically Ill PatientsEward Rod SalNo ratings yet
- 7) 13 AntiepilepticsDocument27 pages7) 13 AntiepilepticsKhushboo IkramNo ratings yet
- CNS PNS DrugsDocument29 pagesCNS PNS DrugsMadel A. AlberioNo ratings yet
- Psychoactive DrugsDocument24 pagesPsychoactive DrugsIshaani GargNo ratings yet
- DMARD'sDocument9 pagesDMARD'sterencedszaNo ratings yet
- Anticonvulsants Power PointDocument146 pagesAnticonvulsants Power Pointrossfancy736No ratings yet
- Neuropharmacology III: Anticonvulsants What Are Seizures?Document6 pagesNeuropharmacology III: Anticonvulsants What Are Seizures?Urugonda VenumadhavNo ratings yet
- Adverse Drug Reaction: Muhammad Faisal NadeemDocument65 pagesAdverse Drug Reaction: Muhammad Faisal NadeemfaisalnadeemNo ratings yet
- Stage 1 Seminar: Clinical Pharmacology of The Nervous SystemDocument38 pagesStage 1 Seminar: Clinical Pharmacology of The Nervous SystemCollin FreemanNo ratings yet
- Pertimbangan Pemilihan Obat Anti Epilepsi DR Nelly Edit 23 JanDocument53 pagesPertimbangan Pemilihan Obat Anti Epilepsi DR Nelly Edit 23 Janvenus002No ratings yet
- A Simplified Guide To Oral Antipsychotic MedicationsDocument20 pagesA Simplified Guide To Oral Antipsychotic MedicationsBruno AlencarNo ratings yet
- FDCDocument10 pagesFDCAnkit PandeyNo ratings yet
- Anti Parkinson Disease - PDF - Pharmacology - AssignmentDocument11 pagesAnti Parkinson Disease - PDF - Pharmacology - AssignmentMr HotmasterNo ratings yet
- Anti Epileptic Drugs - The Old and The New 2011Document10 pagesAnti Epileptic Drugs - The Old and The New 20115stringcelloNo ratings yet
- Toxicology 6Document6 pagesToxicology 6vkm8r5n7h6No ratings yet
- Anti ParkinsonismsDocument7 pagesAnti ParkinsonismsArslan SaeedNo ratings yet
- Epilepsy Update SeshadriDocument10 pagesEpilepsy Update SeshadriSeshadri Sekhar ChatterjeeNo ratings yet
- Objectives:: IndicationsDocument5 pagesObjectives:: IndicationsChrisNo ratings yet
- Emestop PDFDocument6 pagesEmestop PDFDr.2020No ratings yet
- 13 Drugs For Parkinson's DiseaseDocument51 pages13 Drugs For Parkinson's DiseaseJek Dela CruzNo ratings yet
- Medical Treatments For ParkinsonDocument4 pagesMedical Treatments For ParkinsonecwillNo ratings yet
- DiphenhydramineDocument10 pagesDiphenhydramineFebry Dian SinagaNo ratings yet
- Parkinson DiseaseDocument30 pagesParkinson Diseaseseptiman zebuaNo ratings yet
- Treatment of Erectile DysfunctionDocument45 pagesTreatment of Erectile Dysfunctionminnalesri100% (1)
- Drugs Used in Parkinsonism: Functional Circuitry Between The Cortex, Basal Ganglia, and ThalamusDocument5 pagesDrugs Used in Parkinsonism: Functional Circuitry Between The Cortex, Basal Ganglia, and ThalamusHamad AlshabiNo ratings yet
- Epi LepsiDocument29 pagesEpi LepsiGita SerafikaNo ratings yet
- Pharmacology of AntiepilepticDocument36 pagesPharmacology of AntiepilepticManWol JangNo ratings yet
- Antiseizure: Medical University of Sofia, Faculty of Medicine Department of Pharmacology and ToxicologyDocument29 pagesAntiseizure: Medical University of Sofia, Faculty of Medicine Department of Pharmacology and Toxicologybudirahmant0No ratings yet
- Adrenergic AntagonistsDocument23 pagesAdrenergic AntagonistsMirza Shaharyar BaigNo ratings yet
- Antiepileptic Drugs: Department of Pharmacology Zhang Yan-MeiDocument28 pagesAntiepileptic Drugs: Department of Pharmacology Zhang Yan-MeiDrMohammed AlyNo ratings yet
- Lorazepam - Wikipedia, The Free EncyclopediaDocument15 pagesLorazepam - Wikipedia, The Free Encyclopediaapi-18997839No ratings yet
- MontelukastDocument4 pagesMontelukastPrincess Jenelly CampomanesNo ratings yet
- Critical Care Medications: Anti-Arrhythmics Study Guide: Critical Care EssentialsFrom EverandCritical Care Medications: Anti-Arrhythmics Study Guide: Critical Care EssentialsNo ratings yet
- 01.linear CKT Analysis Chp1Document28 pages01.linear CKT Analysis Chp1Sofiane TighiltNo ratings yet
- Engineering Design and Economics Homework 5Document10 pagesEngineering Design and Economics Homework 5Sofiane TighiltNo ratings yet
- Biology O Level October/November 2009Document12 pagesBiology O Level October/November 2009Sofiane Tighilt0% (1)
- Biology O Level October/November 2009Document12 pagesBiology O Level October/November 2009Sofiane Tighilt0% (1)
- Food ChemDocument22 pagesFood ChemLee BenesioNo ratings yet
- Sri Isopanisad: Mantra SevenDocument2 pagesSri Isopanisad: Mantra SevenJejixev100% (1)
- Guia Ingles Iv Segunda Unidad Enero 2022Document16 pagesGuia Ingles Iv Segunda Unidad Enero 2022wallpapersNo ratings yet
- How To Write An EssayDocument4 pagesHow To Write An EssayShah BaibrassNo ratings yet
- Maps by Marie - Ange BrayerDocument17 pagesMaps by Marie - Ange BrayerNadia KalaraNo ratings yet
- Civil Law MTDocument28 pagesCivil Law MTKaira Marie CarlosNo ratings yet
- What Is Radionics - Nick FranksDocument3 pagesWhat Is Radionics - Nick Franksambertje12100% (1)
- Joseph Straus - A Principle of Voice Leading in The Music of StravinskyDocument20 pagesJoseph Straus - A Principle of Voice Leading in The Music of StravinskyIliya GramatikoffNo ratings yet
- Practice Paper 3 Level 11 & 10Document6 pagesPractice Paper 3 Level 11 & 10Eugene JosephNo ratings yet
- Manila Standard Today - Friday (November 23, 2012) IssueDocument28 pagesManila Standard Today - Friday (November 23, 2012) IssueManila Standard TodayNo ratings yet
- PP9 Biodiversity of PlantsDocument93 pagesPP9 Biodiversity of PlantsRorisang MotsamaiNo ratings yet
- ReynalD Ocampo ResumeDocument1 pageReynalD Ocampo Resumerawlens studioNo ratings yet
- Roadmap For Bible StudyDocument1 pageRoadmap For Bible Study4gen_3No ratings yet
- Basic Labor and Employment Education CourseDocument9 pagesBasic Labor and Employment Education CourseJennifer Tan Marcial100% (2)
- The 7 Habits of HIGHLY Effective PeopleDocument12 pagesThe 7 Habits of HIGHLY Effective PeopleWahid T. YahyahNo ratings yet
- Top of FormDocument28 pagesTop of Formsybell8No ratings yet
- Assignment On Dam EngineeringDocument2 pagesAssignment On Dam EngineeringChanako DaneNo ratings yet
- WP 1997 - 16 Catherine Marquette-07112007 - 1Document19 pagesWP 1997 - 16 Catherine Marquette-07112007 - 1k1l2d3No ratings yet
- The Five Fundamental Vowel SoundsDocument18 pagesThe Five Fundamental Vowel SoundsAloneNo ratings yet
- Robert Gabriel TranscriptDocument70 pagesRobert Gabriel TranscriptDaily KosNo ratings yet
- Let Reviewer 2017Document40 pagesLet Reviewer 2017Claudene GellaNo ratings yet
- Week 3 Case Digests Page 57Document137 pagesWeek 3 Case Digests Page 57Andrew Mercado NavarreteNo ratings yet
- First Class Dhanbad 2012Document4 pagesFirst Class Dhanbad 2012ihateu1No ratings yet
- Fishing (Story of Seasons - Friends of Mineral Town) - RanchstoryDocument6 pagesFishing (Story of Seasons - Friends of Mineral Town) - RanchstoryWirawan Amirul BahriNo ratings yet
- Tony Robbins NotesDocument3 pagesTony Robbins Notesrationalgaze0% (2)
- Nolasco Labor I CompilationDocument115 pagesNolasco Labor I CompilationNico QuebalNo ratings yet
- Sit774-10 4HDDocument2 pagesSit774-10 4HDR.A Software Programmer'sNo ratings yet