Download as pptx, pdf, or txt
You might also like
- MTS Vocab 2023Document9 pagesMTS Vocab 2023Rahul Chauhan100% (1)
- GCC - Ykone 2023Document50 pagesGCC - Ykone 2023JeanThomasNo ratings yet
- Community Health NursingDocument25 pagesCommunity Health Nursingjhing_tajul83% (6)
- Institute of Engineering: Tribhuvan UniversityDocument41 pagesInstitute of Engineering: Tribhuvan UniversityShooting Star100% (2)
- ISID InfectionGuide Chapter19Document9 pagesISID InfectionGuide Chapter19Hemanth KumarNo ratings yet
- AreenDocument10 pagesAreenTanaka ChadambukaNo ratings yet
- WASH Presentation VCE HHD Oxfam AustraliaDocument16 pagesWASH Presentation VCE HHD Oxfam AustraliamehtaNo ratings yet
- Diarrhea Safe Water Treatment and Storage in The Home: A Practical New Strategy To Prevent Waterborne Disease Mintz E, Reiff F, Tauxe RDocument7 pagesDiarrhea Safe Water Treatment and Storage in The Home: A Practical New Strategy To Prevent Waterborne Disease Mintz E, Reiff F, Tauxe RAmir RuddinNo ratings yet
- The Three Core Functions and Ten Essential Public Health ServicesDocument5 pagesThe Three Core Functions and Ten Essential Public Health ServicesFau Fau DheoboNo ratings yet
- Microbiologic Effectiveness of Hand WashDocument8 pagesMicrobiologic Effectiveness of Hand WashAsad AliNo ratings yet
- Kelesia - Cholera Outbreak in Haiti 2010Document13 pagesKelesia - Cholera Outbreak in Haiti 2010OPGJrNo ratings yet
- Combating Waterborne Disease at The Household LevelDocument36 pagesCombating Waterborne Disease at The Household LevelSTBM IndonesiaNo ratings yet
- Wastewater Reclamation and Reuse: Mark D. SobseyDocument29 pagesWastewater Reclamation and Reuse: Mark D. Sobsey8108295484No ratings yet
- Article On Promoting Hygiene For Healthy SocietyDocument12 pagesArticle On Promoting Hygiene For Healthy SocietykhanapurkarNo ratings yet
- What Is Vibrio Cholerae?Document4 pagesWhat Is Vibrio Cholerae?IncarcaNo ratings yet
- Water, Sanitation, and Hygiene: Some Facts and FiguresDocument2 pagesWater, Sanitation, and Hygiene: Some Facts and FiguresRanjeet AstroNo ratings yet
- Yemen WASH Cluster - Quick Guidance - Cholera - 2024Document6 pagesYemen WASH Cluster - Quick Guidance - Cholera - 2024Wagdi AlhajjNo ratings yet
- Emergency Handbook PDFDocument10 pagesEmergency Handbook PDFTesfuNo ratings yet
- Doh 07Document37 pagesDoh 07Malack ChagwaNo ratings yet
- BHW Training EnvironmentalDocument19 pagesBHW Training EnvironmentalWilma BeraldeNo ratings yet
- E367itzgr Environmental Sanitation Food Safety and ControlDocument121 pagesE367itzgr Environmental Sanitation Food Safety and ControlJulia Ferhyz UyNo ratings yet
- Household Water Treatment: Chlorination-The Safe Water SystemDocument2 pagesHousehold Water Treatment: Chlorination-The Safe Water SystemcurlyjockeyNo ratings yet
- Module 1.1 introduction-WRID Ds 220831Document33 pagesModule 1.1 introduction-WRID Ds 220831harishfollowerrNo ratings yet
- Saiduskkid Public HealthDocument6 pagesSaiduskkid Public HealthSaidu YusufNo ratings yet
- Hygiene Promotion For Household Water Treatment and Safe Storage in EmergenciesDocument13 pagesHygiene Promotion For Household Water Treatment and Safe Storage in EmergenciesOxfamNo ratings yet
- CholeraDocument21 pagesCholeraIris BalinoNo ratings yet
- Press Release On Waterborne Diseases 02052024Document3 pagesPress Release On Waterborne Diseases 02052024ojwakadanNo ratings yet
- Activity 5 2Document4 pagesActivity 5 2Kate MendozaNo ratings yet
- WASH in CampsDocument13 pagesWASH in CampsMohammed AlfandiNo ratings yet
- CPH Water BorneDocument4 pagesCPH Water BorneAryan SanohNo ratings yet
- SanitationDocument40 pagesSanitationJaynes Ann BoaconNo ratings yet
- Water, Sanitation, and Hygiene: Infectious Diseases, 5 (1), 42-52Document1 pageWater, Sanitation, and Hygiene: Infectious Diseases, 5 (1), 42-52realsilverleNo ratings yet
- Acute Diarrhoeal Diseases Assignment: 1. Define Diarrhea and Describe The Types of DiarrheaDocument3 pagesAcute Diarrhoeal Diseases Assignment: 1. Define Diarrhea and Describe The Types of Diarrheasuhas prabhuNo ratings yet
- Urban WasteDocument59 pagesUrban WasteSisay KetemaNo ratings yet
- NCM 104 Handout On EhsDocument5 pagesNCM 104 Handout On EhsJerah Aceron SatorreNo ratings yet
- Standar Minimum Ketahanan Pangan Dan Gizi: Era Catur PrasetyaDocument28 pagesStandar Minimum Ketahanan Pangan Dan Gizi: Era Catur PrasetyaAmirah RNo ratings yet
- The Safe Water SystemDocument20 pagesThe Safe Water SystemAkintoye AsaoluNo ratings yet
- Cholera: Key FactsDocument9 pagesCholera: Key FactsDennis NjorogeNo ratings yet
- Food Microbiology: 6.12 The Richmond Report On The Microbiological Safety of FoodDocument8 pagesFood Microbiology: 6.12 The Richmond Report On The Microbiological Safety of FoodElviana YaputraNo ratings yet
- Lec07 LantagneDocument54 pagesLec07 LantagneMohamed ElsaneeNo ratings yet
- WHO - Drinking-Water Fact SheetDocument5 pagesWHO - Drinking-Water Fact SheetTejinder SinghNo ratings yet
- Key Activities in Rapid AssessmentDocument15 pagesKey Activities in Rapid AssessmentKewkew AzilearNo ratings yet
- Faecal ColiformsDocument4 pagesFaecal ColiformsAndinajiib MusseNo ratings yet
- ACF WASH Manual Chapter 7 AnnexesDocument165 pagesACF WASH Manual Chapter 7 AnnexesAction Against Hunger USA100% (1)
- Drinking Water or Potable Water Is Water of Sufficiently High Quality That Can Be Consumed or Used Without Risk of Immediate or Long Term HarmDocument2 pagesDrinking Water or Potable Water Is Water of Sufficiently High Quality That Can Be Consumed or Used Without Risk of Immediate or Long Term Harmnive123456No ratings yet
- Hygiene Standards BookletDocument13 pagesHygiene Standards BookletDaniel CraciunescuNo ratings yet
- Excreta Disposal - Onsite SystemsDocument34 pagesExcreta Disposal - Onsite SystemsJordanne LevyNo ratings yet
- Journal Pone 0012613Document10 pagesJournal Pone 0012613Sena AniakuNo ratings yet
- Soap Is Not Enough. Handwashing Practicesand Knowledge in Refugee Camps, MabanCounty, South SudanDocument9 pagesSoap Is Not Enough. Handwashing Practicesand Knowledge in Refugee Camps, MabanCounty, South SudaneerhuangaNo ratings yet
- Water Supply in Healthcare FacilitiesDocument27 pagesWater Supply in Healthcare FacilitiesdalfordNo ratings yet
- Acf Gravity Fed System 1 General Information enDocument44 pagesAcf Gravity Fed System 1 General Information enJorge FigulsNo ratings yet
- Community Water Supply and Sanitation (WSEE 3143) : Chapter OneDocument20 pagesCommunity Water Supply and Sanitation (WSEE 3143) : Chapter Onejebril yusufNo ratings yet
- Water Microbiology NE2283Document59 pagesWater Microbiology NE2283Sharifah Nadzirah100% (2)
- Environmental SanitationDocument20 pagesEnvironmental SanitationKarlRash100% (2)
- Blue-Green Algae FactsDocument3 pagesBlue-Green Algae FactsEmma KoryntaNo ratings yet
- Zimbabwe Water Filters Narrative Report FinalDocument8 pagesZimbabwe Water Filters Narrative Report FinalCamille Van NeerNo ratings yet
- Shigellosis Written ReportDocument4 pagesShigellosis Written ReportVincent ManganaanNo ratings yet
- SCHITOSOMIASISDocument8 pagesSCHITOSOMIASISxteph04No ratings yet
- Out of The Tap: Can I Drink That?Document37 pagesOut of The Tap: Can I Drink That?Elvira FicasNo ratings yet
- Global Water Security: Lessons Learnt and Long-Term ImplicationsFrom EverandGlobal Water Security: Lessons Learnt and Long-Term ImplicationsWorld Water CouncilNo ratings yet
- Empty Buckets and Overflowing Pits: Urban Water and Sanitation Reforms in Sub-Saharan Africa – Acknowledging Decline, Preparing for the Unprecedented Wave of DemandFrom EverandEmpty Buckets and Overflowing Pits: Urban Water and Sanitation Reforms in Sub-Saharan Africa – Acknowledging Decline, Preparing for the Unprecedented Wave of DemandNo ratings yet
- PREPPER'S LONG-TERM SURVIVAL GUIDE: Navigating Challenges and Thriving in Uncertain Times (2023 Guide for Beginners)From EverandPREPPER'S LONG-TERM SURVIVAL GUIDE: Navigating Challenges and Thriving in Uncertain Times (2023 Guide for Beginners)No ratings yet
- ECHO HIV Guidelines FinalDocument27 pagesECHO HIV Guidelines FinalhumphrangoNo ratings yet
- How Does A Siphon WorkDocument22 pagesHow Does A Siphon WorkVinothNo ratings yet
- Maternal DeathDocument4 pagesMaternal DeathhumphrangoNo ratings yet
- Polyethylene (PE) SDR-Pressure Rated Tube: Frictional Head Loss ChartDocument1 pagePolyethylene (PE) SDR-Pressure Rated Tube: Frictional Head Loss CharthumphrangoNo ratings yet
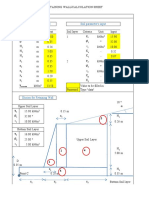
- Retaining Wall's Input Soil Parameter's InputDocument4 pagesRetaining Wall's Input Soil Parameter's Inputhumphrango100% (1)
- PP9 Biodiversity of PlantsDocument93 pagesPP9 Biodiversity of PlantsRorisang MotsamaiNo ratings yet
- Common Object ModelDocument4 pagesCommon Object ModelMahesh AbnaveNo ratings yet
- Top of FormDocument28 pagesTop of Formsybell8No ratings yet
- Austin - A Plea For ExcusesDocument31 pagesAustin - A Plea For ExcusesexactedNo ratings yet
- Certificate & Acknowledgment.Document5 pagesCertificate & Acknowledgment.Ravindra ThakurNo ratings yet
- Ch08 - Principles of Capital InvestmentDocument7 pagesCh08 - Principles of Capital InvestmentStevin GeorgeNo ratings yet
- Forced Air Accessories: Condensate Drain PansDocument16 pagesForced Air Accessories: Condensate Drain PansKamal AliyevNo ratings yet
- Spheciospongia Vesparium, Commonly Known As The LoggerheadDocument2 pagesSpheciospongia Vesparium, Commonly Known As The Loggerheadandrew_yeap_2No ratings yet
- Intermediate Accounting - Kieso - Chapter 1Document46 pagesIntermediate Accounting - Kieso - Chapter 1Steffy AmoryNo ratings yet
- The Exhibitionist Issue 1 PDFDocument64 pagesThe Exhibitionist Issue 1 PDFFelipe PrandoNo ratings yet
- Kainrath Case StudyDocument16 pagesKainrath Case Studyapi-309189621No ratings yet
- Farm Input Marketting System - Arusha PresentationDocument1 pageFarm Input Marketting System - Arusha PresentationFranklin MairuraNo ratings yet
- PCS GSM PicoCell Booster Updated R5 PDFDocument3 pagesPCS GSM PicoCell Booster Updated R5 PDFpandavision76No ratings yet
- S.S.C Public Examination: Model Paper-1 General Science Paper - 1Document4 pagesS.S.C Public Examination: Model Paper-1 General Science Paper - 1Dhatri Subasri Navya KNo ratings yet
- Llorente vs. LlorenteDocument1 pageLlorente vs. LlorenteJen Agustin MalamugNo ratings yet
- Lesson Plan DifferentiationDocument2 pagesLesson Plan Differentiationapi-661625073No ratings yet
- Group 1 Presentors Media and Digital LiteracyDocument28 pagesGroup 1 Presentors Media and Digital LiteracyJOHNERROL CARCELLARNo ratings yet
- Schunk, 2001. Self-Regulation Through Goal SettingDocument4 pagesSchunk, 2001. Self-Regulation Through Goal SettingNani Maciel100% (1)
- Introduction To OB and Individual Work BehaviorDocument14 pagesIntroduction To OB and Individual Work Behaviorphamhuynh nhulyNo ratings yet
- Adverb of Affirmation and Negation Worksheet 3Document6 pagesAdverb of Affirmation and Negation Worksheet 3MARIZ BALBANo ratings yet
- Practice Paper 3 Level 11 & 10Document6 pagesPractice Paper 3 Level 11 & 10Eugene JosephNo ratings yet
- Chapter 3 Lesson 1Document64 pagesChapter 3 Lesson 1Catherine PilipasNo ratings yet
- The A To Z List of Reflexology Research3Document110 pagesThe A To Z List of Reflexology Research3Ahmad Saiful Ridzwan JaharuddinNo ratings yet
- 7 ChakrasDocument36 pages7 ChakrasmadhulataagiwalNo ratings yet
- Ratio Analysis ProjectDocument63 pagesRatio Analysis ProjectYalluraj HukkeriNo ratings yet
- ENG 401 VU Lecture 5Document16 pagesENG 401 VU Lecture 5ImranNo ratings yet
- Improper Landscapes of Desire: Alternative Routes Towards (Un) Satisfaction in The Narrative of Ena Lucía PortelaDocument10 pagesImproper Landscapes of Desire: Alternative Routes Towards (Un) Satisfaction in The Narrative of Ena Lucía PortelayunlectorNo ratings yet




























































![Sewage and sewerage of farm homes [1928]](https://imgv2-1-f.scribdassets.com/img/word_document/544942443/149x198/ae3275e6b6/1676295883?v=1)