Download as ppt, pdf, or txt
You might also like
- Psychiatry Study Guide For ShelfDocument42 pagesPsychiatry Study Guide For Shelfappolinia64% (14)
- DLP q1 P.E 8Document25 pagesDLP q1 P.E 8Riz Monterola100% (6)
- Bipolar 1 and Bipolar 2Document27 pagesBipolar 1 and Bipolar 2api-546355187No ratings yet
- Psychiatry Pharmacology J. Psychiatry' AntidepressantsDocument9 pagesPsychiatry Pharmacology J. Psychiatry' AntidepressantssumithjalyNo ratings yet
- Bipolar DisorderDocument22 pagesBipolar Disorderpharmacist2008100% (9)
- Mood DisorderDocument6 pagesMood DisorderHilton D. CalawenNo ratings yet
- Pharmacology of Mood Stabilizers: DR - Datten Bangun, MSC, SPFK Dept - Farmakologi & Terapetik Fak - Kedokteran Uhn MedanDocument51 pagesPharmacology of Mood Stabilizers: DR - Datten Bangun, MSC, SPFK Dept - Farmakologi & Terapetik Fak - Kedokteran Uhn MedanFansisca SiallaganNo ratings yet
- Mood Stabilizers-Amanat Ali-1Document33 pagesMood Stabilizers-Amanat Ali-1Syed Sanan shahNo ratings yet
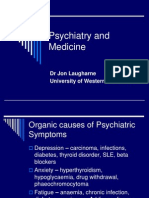
- Psychiatry and Medicine: DR Jon Laugharne University of Western AustraliaDocument22 pagesPsychiatry and Medicine: DR Jon Laugharne University of Western AustralialxnalexanderNo ratings yet
- Mental Health Nursing II NURS 2310Document59 pagesMental Health Nursing II NURS 2310CARTAGENA1No ratings yet
- Antimanic & CNS StimulantDocument40 pagesAntimanic & CNS StimulantSunanda mohanNo ratings yet
- Antidepressants AntidepressantsDocument38 pagesAntidepressants AntidepressantsjaneNo ratings yet
- Endocrine SystemDocument37 pagesEndocrine SystemzeinabNo ratings yet
- Drugs Used To Treat Bipolar Disorder: By: DR Satar OstadhadiDocument31 pagesDrugs Used To Treat Bipolar Disorder: By: DR Satar OstadhadiSattar OstadhadiNo ratings yet
- Emotional Response and Mood DisordersDocument51 pagesEmotional Response and Mood DisordersAnabelle RicoNo ratings yet
- Mood DisorderDocument42 pagesMood DisorderAbdul Razak OthmanNo ratings yet
- Community Paeds, Psychpharm non-ADHD-DEfronDocument53 pagesCommunity Paeds, Psychpharm non-ADHD-DEfronSriraag BalajiNo ratings yet
- Depression & Suicide: DR - Sarath Menon.R Department of Neurology MGM Medical College, IndoreDocument50 pagesDepression & Suicide: DR - Sarath Menon.R Department of Neurology MGM Medical College, IndoreKrishna KanthNo ratings yet
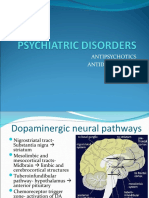
- Psychiatric DisordersDocument23 pagesPsychiatric DisordersRahul PatilNo ratings yet
- Mood Stabilisers by NavinaDocument91 pagesMood Stabilisers by NavinaNavina SureshNo ratings yet
- Antidepressant Drugs: Presented By-K.Vinod Dept. of PharmacologyDocument38 pagesAntidepressant Drugs: Presented By-K.Vinod Dept. of PharmacologyVinod GuruNo ratings yet
- Bipolar Disorder: Dr. Babar Rauf PG Trainee Anesthesia, BBH, RawalpindiDocument11 pagesBipolar Disorder: Dr. Babar Rauf PG Trainee Anesthesia, BBH, RawalpindiBabar RaufNo ratings yet
- AntipsychoticsDocument4 pagesAntipsychoticsRana MuhammadNo ratings yet
- 7) 5th Semester - Depression & Affective DisordersDocument33 pages7) 5th Semester - Depression & Affective DisordersFizza ImamNo ratings yet
- Drugs For Psychiatric DisordersDocument59 pagesDrugs For Psychiatric DisordersQodriyah HmsNo ratings yet
- Peak Onset: 16 - 20 Years Old: Eating DisorderDocument3 pagesPeak Onset: 16 - 20 Years Old: Eating DisorderAnnie ChaoNo ratings yet
- 22 Psychotherapeutic AgentsDocument5 pages22 Psychotherapeutic AgentsAngel HannahNo ratings yet
- Mental Disorders Due To A General Medical ConditionDocument145 pagesMental Disorders Due To A General Medical ConditionKaye NepomucenoNo ratings yet
- Mood Disorders: C. Baker-Burke MSCN, BSCN, RNDocument39 pagesMood Disorders: C. Baker-Burke MSCN, BSCN, RNObrian ReidNo ratings yet
- ManiaDocument10 pagesManiaRizky Dwidya AmirtasariNo ratings yet
- 1n2 OrganicSD-drshakyaDocument26 pages1n2 OrganicSD-drshakyaUMESH KANDELNo ratings yet
- Pharmacology in PsychiatryDocument33 pagesPharmacology in PsychiatryKatrina PonceNo ratings yet
- 2n2 OrganicSD-drshakyaDocument20 pages2n2 OrganicSD-drshakyaUMESH KANDELNo ratings yet
- Psychiatrypoisoning E.ODocument24 pagesPsychiatrypoisoning E.OZeenat JunaidNo ratings yet
- Substance Abuse Power PointDocument65 pagesSubstance Abuse Power PointFletcher1980No ratings yet
- AntidepressantsDocument5 pagesAntidepressantsUm HamoOd100% (2)
- What To Know On The Exam: Mania - 7 QuestionsDocument11 pagesWhat To Know On The Exam: Mania - 7 QuestionsNyein Nu WinnNo ratings yet
- Pharmacology 402 February 24, 2010 Mark Hamblin, MD, PHDDocument54 pagesPharmacology 402 February 24, 2010 Mark Hamblin, MD, PHDKarmila Novianti100% (1)
- Drug Studies (Levodopa, Ropinirole, Rivastigmine Tatrate, Glucerna)Document12 pagesDrug Studies (Levodopa, Ropinirole, Rivastigmine Tatrate, Glucerna)KBDNo ratings yet
- Mood-Stabilizing AgentsDocument9 pagesMood-Stabilizing AgentsRoci ArceNo ratings yet
- Randa Al-Harizy Prof of Internal MedicineDocument40 pagesRanda Al-Harizy Prof of Internal MedicinerafikaNo ratings yet
- ANTIDEPRESSANTS MaterialDocument5 pagesANTIDEPRESSANTS MaterialxyzNo ratings yet
- Antidepressants MaterialDocument5 pagesAntidepressants MaterialxyzNo ratings yet
- PsychopharmacologyDocument84 pagesPsychopharmacologyKhyra Ysabelle VillanuevaNo ratings yet
- Bipolar Disorders PowerpointDocument14 pagesBipolar Disorders PowerpointjoycechicagoNo ratings yet
- NeuropharmacologyDocument30 pagesNeuropharmacologytracy_lau_8No ratings yet
- Lithium Final 2Document42 pagesLithium Final 2Neha PashineNo ratings yet
- Psych MedicationsDocument6 pagesPsych Medicationsash00se7enNo ratings yet
- Alcohol Use Disorder 2Document176 pagesAlcohol Use Disorder 2Priyanka KoundinyaNo ratings yet
- AntiepilepticsDocument52 pagesAntiepilepticsAkshay NirwalNo ratings yet
- Assessment & Specific Managements: Alcohol UseDocument34 pagesAssessment & Specific Managements: Alcohol UseChris Jardine LiNo ratings yet
- AntidepressantsDocument36 pagesAntidepressantsLloyd Daniel BarrantesNo ratings yet
- Psycho PharmaDocument8 pagesPsycho PharmaMark JosephNo ratings yet
- AntidepressantsDocument4 pagesAntidepressantsSalman HabeebNo ratings yet
- Joana Marie E. Gantuangco: Harrison's 20th EditionDocument27 pagesJoana Marie E. Gantuangco: Harrison's 20th EditionJoana Marie Gantuangco-MaglinteNo ratings yet
- Bipolar Disorder: Presented by Dr. Chandan N Intern, Department of Psychiatry, MIMS, MandyaDocument23 pagesBipolar Disorder: Presented by Dr. Chandan N Intern, Department of Psychiatry, MIMS, MandyaSiddharth MalikNo ratings yet
- Tanveer A Padder MD Medical Director Optimum Health & MPB Group MarylandDocument172 pagesTanveer A Padder MD Medical Director Optimum Health & MPB Group MarylandtpadderNo ratings yet
- Psychotherapist'S Guide To Psychopharmacology: Second EditionFrom EverandPsychotherapist'S Guide To Psychopharmacology: Second EditionRating: 5 out of 5 stars5/5 (6)
- Depression and Bipolar Disorder: Your Guide to RecoveryFrom EverandDepression and Bipolar Disorder: Your Guide to RecoveryRating: 4.5 out of 5 stars4.5/5 (3)
- The Maudsley Prescribing Guidelines in PsychiatryFrom EverandThe Maudsley Prescribing Guidelines in PsychiatryRating: 5 out of 5 stars5/5 (1)
- Hepatic Encephalopathy, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHepatic Encephalopathy, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsRating: 4 out of 5 stars4/5 (1)
- Vestige E-Catalogue India - August 2021Document145 pagesVestige E-Catalogue India - August 2021SamyamoyNo ratings yet
- SuboxonecenterbriefDocument5 pagesSuboxonecenterbriefapi-314460549No ratings yet
- Self-Declaration Form - STUDIODocument2 pagesSelf-Declaration Form - STUDIOLeticia BikaerNo ratings yet
- New Frontiers of Genetics and The Risk of EugenicsDocument132 pagesNew Frontiers of Genetics and The Risk of EugenicsOscar Sanchez CarreñoNo ratings yet
- Sport Dissertation Topic IdeasDocument8 pagesSport Dissertation Topic IdeasWritingPaperHelpSingapore100% (1)
- Pengambilan Keputusan Klinis Perawat: Jurnal Ilmiah Kesehatan 2020Document11 pagesPengambilan Keputusan Klinis Perawat: Jurnal Ilmiah Kesehatan 2020Dafarasyad DafarasyadNo ratings yet
- 0 - Reflection MCNDocument1 page0 - Reflection MCNVanessa Mae IlaganNo ratings yet
- Critical Appraisal Checklist For An Article OnDocument4 pagesCritical Appraisal Checklist For An Article OnTiaz DiniutamiNo ratings yet
- Important Questions Answers Why This Matters:: (G4056/P2509) (G4057/P2509)Document8 pagesImportant Questions Answers Why This Matters:: (G4056/P2509) (G4057/P2509)JskNo ratings yet
- MCN Drill 1Document23 pagesMCN Drill 1Cai Velasco DecenaNo ratings yet
- Birth StoryDocument7 pagesBirth StoryKaty Whipple100% (1)
- Ebook Braddoms Physical Medicine and Rehabilitation Sixth Edition PDF Full Chapter PDFDocument67 pagesEbook Braddoms Physical Medicine and Rehabilitation Sixth Edition PDF Full Chapter PDFmelinda.warren862100% (34)
- Laporan IKM KSM PK FEBRUARI 2022Document27 pagesLaporan IKM KSM PK FEBRUARI 2022Nur iffahNo ratings yet
- Infective EndocarditisDocument18 pagesInfective EndocarditisLee Foo WengNo ratings yet
- Reviste Medicale Internationale Cotate IsiDocument28 pagesReviste Medicale Internationale Cotate IsidoruNo ratings yet
- Bag TechniqueDocument5 pagesBag Techniqueamp_raphNo ratings yet
- USOR Annual Report 2011Document54 pagesUSOR Annual Report 2011State of UtahNo ratings yet
- Hong Kong's First Professor of Pathology and The Laboratory of The Royal College of Physicians of EdinburghDocument6 pagesHong Kong's First Professor of Pathology and The Laboratory of The Royal College of Physicians of EdinburghJhonalValdimirQuispeMamaniNo ratings yet
- Module 3 Emergency Preparedness and Response ManagementDocument13 pagesModule 3 Emergency Preparedness and Response ManagementMa. AlbinaNo ratings yet
- Codependency Treatment Systematic Review 2015Document12 pagesCodependency Treatment Systematic Review 2015Ryan PetersonNo ratings yet
- Thesis Parkinson DiseaseDocument8 pagesThesis Parkinson Diseaseaouetoiig100% (1)
- BPQY Release 90808 #1Document1 pageBPQY Release 90808 #1Terry PetersonNo ratings yet
- Presentasi Jurnal Stase Keperawatan Medikal BedahDocument17 pagesPresentasi Jurnal Stase Keperawatan Medikal BedahDellia WinadaNo ratings yet
- Bipolar Disorder Effects On The FamilyDocument2 pagesBipolar Disorder Effects On The FamilyAlina LunguNo ratings yet
- Nanotechnology For Biomedical ApplicationsDocument15 pagesNanotechnology For Biomedical ApplicationsVanitha AlagarsamyNo ratings yet
- Intussuseption and Hirschprung's DiseaseDocument5 pagesIntussuseption and Hirschprung's DiseaseAris Magallanes100% (2)
- CSH Guidelines For The Diagnosis and Treatment of Drug-Induced Liver InjuryDocument21 pagesCSH Guidelines For The Diagnosis and Treatment of Drug-Induced Liver InjuryIndraNo ratings yet
- Checked Testing Effectiveness of Types of ToothpasteDocument9 pagesChecked Testing Effectiveness of Types of ToothpasteMaya AltahaNo ratings yet
- AIDS Foundation of Chicago - Annual Report 2015Document24 pagesAIDS Foundation of Chicago - Annual Report 2015AdamAce VelasquezNo ratings yet